Cms-L564 Printable Form
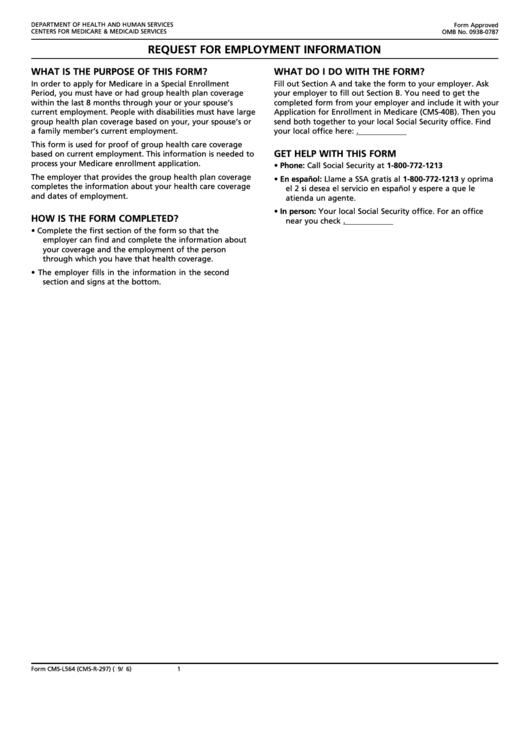
Cms-L564 Printable Form - Sign up for part a. Name, address and phone number. Social security administration telephone number: Web your employer doesn’t need to sign section b of the cms l564 form. Find your local office here: If you don’t already have part a. National provider identifier (npi) application/update form. Web fill out section a and take the form to your employer. State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application. Web if you have comments concerning the accuracy of the time estimate (s) or suggestions for improving this form, please write to:
Sign up for part a. State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application. If you don’t already have part a. Cms, 7500 security boulevard, attn: Department of health and human services centers for medicare & medicaid services form approved omb no. Name, address and phone number. Then you send both together to your local social security office. Find your local office here: Web fill out section a and take the form to your employer. Social security administration telephone number:
Name, address and phone number. Find your local office here: Ask your employer to fill out section b. Then you send both together to your local social security office. Social security administration telephone number: If you don’t already have part a. Web if you have comments concerning the accuracy of the time estimate (s) or suggestions for improving this form, please write to: State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application. Department of health and human services centers for medicare & medicaid services form approved omb no. National provider identifier (npi) application/update form.
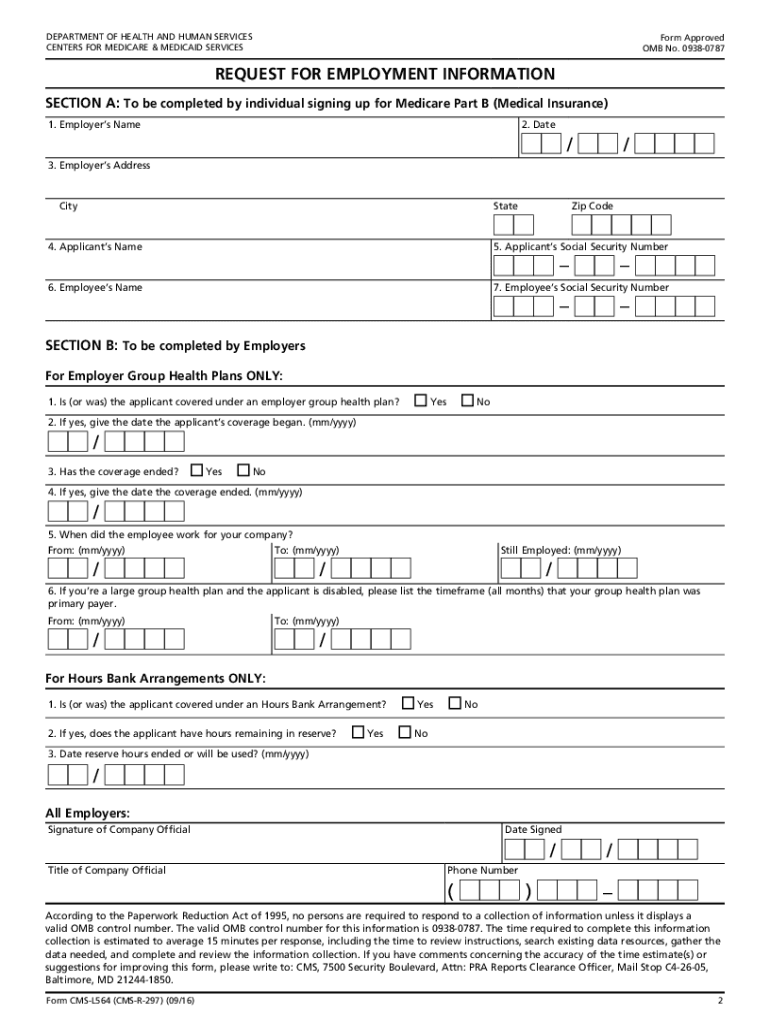
Fillable Form CmsL564 (CmsR297) Request For Employment Information
Web if you have comments concerning the accuracy of the time estimate (s) or suggestions for improving this form, please write to: Sign up for part a. Find your local office here: Cms, 7500 security boulevard, attn: Ask your employer to fill out section b.
Cms l564 cms r Fill out & sign online DocHub
If you don’t already have part a. State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application. Web fill out section a and take the form to your employer. Web your employer doesn’t need to sign section b of the cms l564 form. Department of health and human.
Medicare Part B Enrollment Form Cms L564 Form Resume Examples
National provider identifier (npi) application/update form. Web if you have comments concerning the accuracy of the time estimate (s) or suggestions for improving this form, please write to: Department of health and human services centers for medicare & medicaid services form approved omb no. Then you send both together to your local social security office. Ask your employer to fill.
20162021 Form CMSL564 Fill Online, Printable, Fillable, Blank pdfFiller
Department of health and human services centers for medicare & medicaid services form approved omb no. Cms, 7500 security boulevard, attn: Web your employer doesn’t need to sign section b of the cms l564 form. Social security administration telephone number: Then you send both together to your local social security office.
Form CMS20134 Download Fillable PDF or Fill Online Medicare Enrollment
Web fill out section a and take the form to your employer. Ask your employer to fill out section b. Web your employer doesn’t need to sign section b of the cms l564 form. Name, address and phone number. Cms, 7500 security boulevard, attn:
Form cms l564 for retired federal employees opm Fill out & sign online
Ask your employer to fill out section b. Sign up for part a. If you don’t already have part a. Then you send both together to your local social security office. Name, address and phone number.

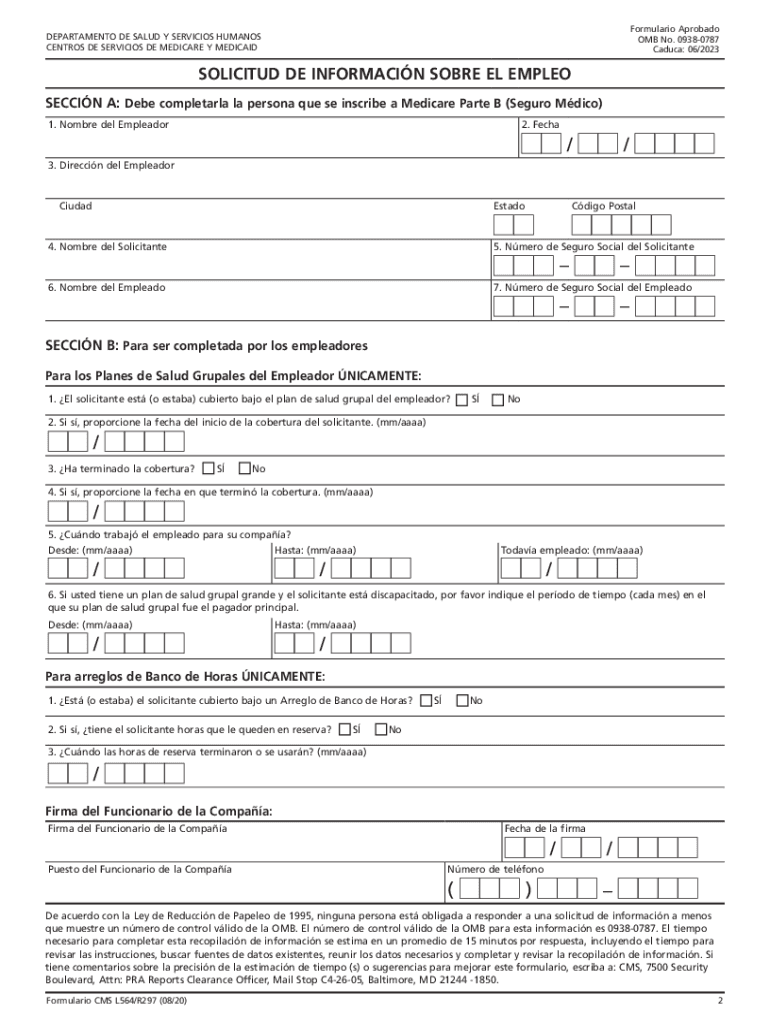
Formulario CMSL564 Download Fillable PDF or Fill Online Solicitud De
Find your local office here: Department of health and human services centers for medicare & medicaid services form approved omb no. Ask your employer to fill out section b. Social security administration telephone number: Web your employer doesn’t need to sign section b of the cms l564 form.

Medicare Part B Application Form Cms L564 Form Resume Examples
Sign up for part a. Then you send both together to your local social security office. Name, address and phone number. State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application. Cms, 7500 security boulevard, attn:

Medicare Part B Application Form Cms L564 Universal Network
National provider identifier (npi) application/update form. Cms, 7500 security boulevard, attn: Web fill out section a and take the form to your employer. Find your local office here: State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application.
Medicare Part B Form Cms L564 Form Resume Examples MeVRB6DzVD
Then you send both together to your local social security office. Social security administration telephone number: Cms, 7500 security boulevard, attn: Find your local office here: Department of health and human services centers for medicare & medicaid services form approved omb no.
Cms, 7500 Security Boulevard, Attn:
Then you send both together to your local social security office. Name, address and phone number. Find your local office here: State “i want part b coverage to begin (mm/yy)” in the remarks section of the cms 40b form or the online application.
If You Don’t Already Have Part A.
Sign up for part a. Web your employer doesn’t need to sign section b of the cms l564 form. Web if you have comments concerning the accuracy of the time estimate (s) or suggestions for improving this form, please write to: National provider identifier (npi) application/update form.
Ask Your Employer To Fill Out Section B.
Department of health and human services centers for medicare & medicaid services form approved omb no. Social security administration telephone number: Web fill out section a and take the form to your employer.